

Background Unplanned 30-day readmissions are a frequent complication of acute leukemia therapy. However, there is limited data in acute lymphoblastic leukemia (ALL), with reported readmission rates (RaR) of 36% for pediatric ALL.
Methods We retrospectively reviewed hospitalizations for ALL for adult patients >/= 18 years at our institution between January 2018 and December 2018. Unplanned readmissions were defined as any hospitalization within 30-days after discharge from the index admission, excluding all elective re-admissions for scheduled chemotherapy. Patients >/= 55 years of age receiving their initial induction therapy remained hospitalized for at least 21 days until bone marrow analysis and neutrophil count above 500/mm3.
The primary objective was to identify the 30-day unplanned readmission rates, cause of readmissions, and predicted factors for readmissions. The secondary outcome included 30-day readmission mortality rate and inpatient mortality rate.
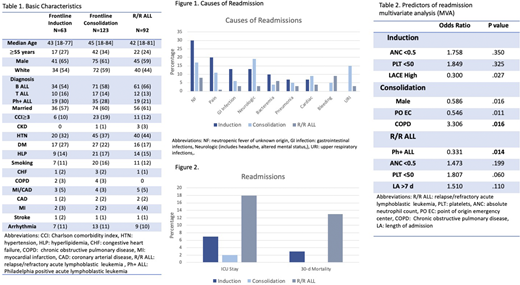
Results There were a total of 841 ALL hospitalizations, 94 admissions for 63 pts (average 1.49 re-admit/pt) during frontline induction, 443 for 123 pts (average 3.6) during consolidation and 304 for 92 pts (average 3.3) with relapsed/refractory ALL (R/R ALL). The median age was 43 years for the frontline induction, 45 years for the consolidation group, and 42 years for R/R ALL patients. Baseline characteristics are listed in Table 1. The median length of index admission was 11 days for induction, 4 days during consolidation, and 8 days for R/R ALL. The 30-day unplanned RaR was 32% for induction, 28% for consolidation, and 36% for R/R ALL, with a median time to readmission of 6 days, 6 days, and 5 days, respectively.
The most common causes of readmissions were infections (60%, 60% and 29% during induction, consolidation and R/R ALL respectively), including 30% neutropenic fever of unknown origin (NF), pain 20%, gastrointestinal infections 13%, neurologic causes (altered mental status, headache and LE weakness) 13%, and 10% bacteremia for induction; 19% neurologic causes, 17% NF, 15% upper respiratory infections, and11% pain during consolidation; and 9% bleeding, 8% NF, and 6% bacteremia for R/R ALL. (Figure 1)
The median length of readmission was 5 days, 4 days, and 7 days for induction, consolidation, and R/R ALL patients, with a rate of ICU stay of 7%, 2%, and 18%, respectively. (Figure 2)
While no significant differences were seen in the rate of ICU stay between readmissions and non-readmission for the induction and consolidation groups, R/R ALL patients had an increased incidence of ICU stay (18% vs. 11%, p=.001) and 30-day mortality (13% vs. 5% p=.010).
We performed a logistical regression analysis to determine risk factors associated with readmissions. The multivariate analysis identified COPD (OR 3.30, p=.016) as an independent predictor for readmissions and male sex was associated with a decreased risk (OR 0.58, p=.016) during consolidation therapy; meanwhile, Philadelphia positive ALL (Ph+ALL) was negatively associated with RaR for R/R ALL pts (OR 0.33, p=.014). (Table 2) There was no significant association between the commonly used L.A.C.E. score and the risk of readmissions among consolidation and R/R ALL pts. However, during induction, a higher L.A.C.E score was negatively associated with the risk of readmission (OR 0.30, p=.027), likely due to a longer duration of hospital stay for high-risk patients (18 days vs. 8 days, p=.000).
The 30-day mortality rate and inpatient mortality rate was 3% for unplanned induction readmissions, 0% for consolidation, and 13% for R/R ALL. One patient (3%) died after readmission during induction due to infection. The 30-day mortality rate after readmission for R/R ALL patients was 13%, with 50% of deaths due to infections and 30% due to disease progression.
Conclusions Unplanned 30-day readmissions were frequent among patients with ALL, with similar rates between each sequential line of therapy, and the most common cause was infections. The 30-day mortality remains low for induction and consolidation pts, with a significantly higher risk for ICU stay and 30-day mortality for R/R ALL pts. We identified COPD, female sex, and non-Ph+ ALL as independent predictors for readmission. However, the majority of the pts were younger, with only 24-34% above 55 years of age. Implementing more frequent monitoring and increased precautions in high-risk pts could help reduce mortality in ALL.
Jain:Aprea Therapeutics: Research Funding; Janssen: Honoraria, Membership on an entity's Board of Directors or advisory committees; ADC Therapeutics: Research Funding; Precision Bioscienes: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Incyte: Research Funding; Adaptive Biotechnologies: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; AbbVie: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Cellectis: Research Funding; Fate Therapeutics: Research Funding; BeiGene: Honoraria, Membership on an entity's Board of Directors or advisory committees; AstraZeneca: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Genentech: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Pharmacyclics: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Verastem: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Servier: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; TG Therapeutics: Honoraria, Membership on an entity's Board of Directors or advisory committees; BMS: Research Funding; Pfizer: Research Funding. Short:AstraZeneca: Consultancy; Astellas: Research Funding; Amgen: Honoraria; Takeda Oncology: Consultancy, Honoraria, Research Funding. Ravandi:Celgene: Consultancy, Honoraria; Orsenix: Consultancy, Honoraria, Research Funding; Abbvie: Consultancy, Honoraria, Research Funding; BMS: Consultancy, Honoraria, Research Funding; Amgen: Consultancy, Honoraria, Research Funding; Astellas: Consultancy, Honoraria, Research Funding; Macrogenics: Research Funding; Xencor: Consultancy, Honoraria, Research Funding; AstraZeneca: Consultancy, Honoraria; Jazz Pharmaceuticals: Consultancy, Honoraria, Research Funding. Borthakur:Abbvie: Research Funding; Curio Science LLC: Consultancy; Polaris: Research Funding; Jannsen: Research Funding; PTC Therapeutics: Consultancy; Argenx: Consultancy; PTC Therapeutics: Research Funding; GSK: Research Funding; FTC Therapeutics: Consultancy; Treadwell Therapeutics: Consultancy; BMS: Research Funding; AstraZeneca: Research Funding; Novartis: Research Funding; Incyte: Research Funding; Cyclacel: Research Funding; BioLine Rx: Consultancy; Xbiotech USA: Research Funding; BioLine Rx: Research Funding; Oncoceutics: Research Funding; BioTherix: Consultancy; Nkarta Therapeutics: Consultancy. Sasaki:Daiichi Sankyo: Consultancy; Novartis: Consultancy, Research Funding; Pfizer Japan: Consultancy; Otsuka: Honoraria. Cortes:Novartis: Consultancy, Research Funding; Merus: Research Funding; Immunogen: Research Funding; Bristol-Myers Squibb: Research Funding; Daiichi Sankyo: Consultancy, Research Funding; Amphivena Therapeutics: Research Funding; Arog: Research Funding; BiolineRx: Consultancy, Research Funding; Sun Pharma: Research Funding; Astellas: Research Funding; Telios: Research Funding; BioPath Holdings: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Pfizer: Consultancy, Research Funding; Jazz Pharmaceuticals: Consultancy, Research Funding; Takeda: Consultancy, Research Funding. Kantarjian:Actinium: Honoraria, Membership on an entity's Board of Directors or advisory committees; Agios: Honoraria, Research Funding; Ariad: Research Funding; Amgen: Honoraria, Research Funding; Takeda: Honoraria; AbbVie: Honoraria, Research Funding; BMS: Research Funding; Novartis: Research Funding; Astex: Research Funding; Daiichi-Sankyo: Research Funding; Immunogen: Research Funding; Pfizer: Honoraria, Research Funding; Cyclacel: Research Funding; Jazz Pharma: Research Funding. Garcia-Manero:AbbVie: Honoraria, Research Funding; Acceleron Pharmaceuticals: Consultancy, Honoraria; Celgene: Consultancy, Honoraria, Research Funding; Helsinn Therapeutics: Consultancy, Honoraria, Research Funding; Novartis: Research Funding; Merck: Research Funding; Astex Pharmaceuticals: Consultancy, Honoraria, Research Funding; Jazz Pharmaceuticals: Consultancy; Bristol-Myers Squibb: Consultancy, Research Funding; Genentech: Consultancy, Membership on an entity's Board of Directors or advisory committees, Research Funding; Onconova: Research Funding; H3 Biomedicine: Research Funding; Amphivena Therapeutics: Research Funding. Jabbour:AbbVie: Other: Advisory role, Research Funding; Pfizer: Other: Advisory role, Research Funding; BMS: Other: Advisory role, Research Funding; Amgen: Other: Advisory role, Research Funding; Genentech: Other: Advisory role, Research Funding; Takeda: Other: Advisory role, Research Funding; Adaptive Biotechnologies: Other: Advisory role, Research Funding. Kadia:Incyte: Research Funding; Celgene: Research Funding; Cellenkos: Research Funding; Genentech: Honoraria, Research Funding; JAZZ: Honoraria, Research Funding; Cyclacel: Research Funding; Novartis: Honoraria; Pulmotec: Research Funding; Abbvie: Honoraria, Research Funding; Ascentage: Research Funding; Astra Zeneca: Research Funding; Amgen: Research Funding; Pfizer: Honoraria, Research Funding; BMS: Honoraria, Research Funding; Astellas: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal